Introduction
Acute coronary syndrome (ACS) refers to the spectrum of clinical presentations ranging from ST-segment elevation myocardial infarction (STEMI) to non–ST-segment elevation myocardial infarction (NSTEMI) to unstable angina (ie, acute coronary syndrome without release of enzymes or biomarkers of myocardial necrosis).
In terms of pathology, acute coronary syndrome is almost always associated with rupture of an atherosclerotic plaque and partial or complete thrombosis of the infarct-related artery. However, in some instances, stable coronary artery disease (CAD) may result in acute coronary syndrome in the absence of plaque rupture and thrombosis when physiologic stress (eg, trauma, blood loss, anemia, infection, tachyarrhythmias) increases demands on the heart.
The diagnosis of acute myocardial infarction in this setting requires a finding of the typical rise and fall of biochemical markers of myocardial necrosis in addition to at least 1 of the following: ischemic symptoms, development of pathologic Q waves, ischemic ST-segment changes on ECG or in the setting of a coronary intervention.1 Therefore, presence of appropriate symptoms in temporal relation to rise and fall in cardiac enzymes constitutes acute myocardial infarction even if typical ischemic ECG changes are absent. On the other hand, a minimal rise in troponin levels in a patient with renal failure is insufficient to diagnose acute myocardial infarction if symptoms and/or ECG changes are absent.
The terms transmural and nontransmural (subendocardial) myocardial infarction are no longer used because ECG findings in patients with this condition are not closely correlated with pathologic changes in the myocardium. Therefore, a transmural infarct may occur in the absence of Q waves on ECGs, and many Q-wave myocardial infarctions may be subendocardial, as noted on pathologic examination. Because elevation of the ST segment during acute coronary syndrome is correlated with coronary occlusion and because it affects the choice of therapy (urgent reperfusion therapy), ACS-related myocardial infarction should be designated STEMI or NSTEMI.
This article focuses on non–ST-elevation acute coronary syndrome. Patients with a new or presumed new left bundle-branch block are also excluded from the discussion below because they are regarded as having ST-elevation acute coronary syndrome and treated accordingly.
Key points of discussion include the following:
- Increasing public awareness of the typical and atypical presentations of acute coronary syndrome is of utmost importance for optimal and timely treatment. Many patients do not recognize that their symptoms are cardiac in origin, and they delay seeking medical help. Guidelines from the European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA) recommend that patients with established coronary artery disease call emergency medical services if they have chest pain that does not resolve after they take a sublingual nitroglycerin tablet.
- An ECG obtained by emergency medical services personnel in the field can be helpful in making an early diagnosis of myocardial ischemia.
- Immediate triage and obtaining a 12-lead ECG within a few minutes of the patient's arrival to the emergency department are extremely important in initially determining the patient's risk category.
- Further early risk stratification depends on the patient's clinical history, findings on physical examination, repeat ECG results, and results of blood work including markers of myocardial damage.
- NSTEMI is distinguished from unstable angina by elevated levels of cardiac enzymes and biomarkers of myocyte necrosis. Differentiation is generally based on 3 sets of biomarkers measured at 6- to 8-hour intervals after the patient's presentation to ED. The current definition of NSTEMI requires a typical clinical syndrome plus elevated troponin (or creatine kinase isoenzyme MB [CK-MB]) levels to >99% of the normal reference (with a coefficient of variation of <10%>
For related information, see eMedicine articles Unstable Angina and Myocardial Infarction.
Pathophysiology
Atherosclerosis is primarily responsible for acute coronary syndrome. Most cases of acute coronary syndrome occur from disruption of a previously nonsevere lesion (an atherosclerotic lesion that was previously hemodynamically insignificant yet vulnerable to rupture). The vulnerable plaque is typified by a large lipid pool, numerous inflammatory cells, and a thin fibrous cap. New modalities, such as optical coherence tomography (OCT), palpography, and virtual histology, are being studied to identify vulnerable plaques.
The major trigger for coronary thrombosis is considered to be plaque rupture caused by the dissolution of the fibrous cap due to the release of metalloproteinases (collagenases) from activated inflammatory cells. This event is followed by platelet activation and aggregation, activation of the coagulation pathway, and vasoconstriction. This process culminates in coronary intraluminal thrombosis and variable degrees of vascular occlusion. Distal embolization may occur. The severity and duration of coronary arterial obstruction, the volume of myocardium affected, the level of demand, and the ability of the rest of the heart to compensate are major determinants of a patient's clinical presentation and outcome.
Demand influences acute coronary syndrome due to increased myocardial oxygen and nutrition requirements (such as exertion, emotional stress, or physiologic stress such as dehydration, blood loss, hypotension, infection, thyrotoxicosis, and surgery). Anemia and hypoxemia can precipitate myocardial ischemia in the absence of severe reduction in coronary artery blood flow. Elevated demand can produce acute coronary syndrome in the presence of a high-grade fixed coronary obstruction. Acute coronary syndrome without elevation in demand requires a new impairment in supply, typically due to thrombosis and/or plaque hemorrhage.
A syndrome consisting of chest pain, ischemic ST-segment and T-wave changes, elevated levels of biomarkers of myocyte injury, and transient left ventricular apical ballooning (takotsubo syndrome) has been shown to occur in the absence of clinical coronary artery disease, after emotional or physical stress. The pathogenesis of this syndrome is not well understood but is thought to relate to a surge of catechol stress hormones and/or high sensitivity to those hormones.
Attention to the underlying pathophysiologic mechanisms of ischemia is important when managing acute coronary syndrome. A simple predictor of demand is rate-pressure product, which can be lowered by beta blockers (eg, metoprolol or atenolol) and pain/stress relievers (eg, morphine), while supply may be improved by oxygen, adequate hematocrit, blood thinners (eg, heparin, IIb/IIIa agents such as abciximab, eptifibatide, tirofiban, or thrombolytics) and/or vasodilators (eg, nitrates, amlodipine). Recently, ranolazine2 was released as a new agent that slows fast channel activity in diastole and provides an additional means to treat angina, but it has risk of QT prolongation and its inclusion for acute coronary syndrome treatment did not reduce the risk of major cardiovascular events such as death, heart attack, or recurrent ischemia.
Frequency, Mortality and Morbidity, Sex, Age, and Race
Frequency
In the United States, approximately 1.7 million cases of acute coronary syndrome were diagnosed in 2001. Rates of first-listed admission diagnosis of unstable angina fell 87% from 29.7/10,000 in 1988 to 3.9/10,000 in 2001 for all age and sex groups, and rates of acute coronary syndrome as a primary diagnosis declined 44%.
Internationally, cardiovascular diseases cause 12 million deaths throughout the world each year, according to the third monitoring report of the World Health Organization, 1991-1993. Cardiovascular disease causes almost half of all deaths in the developed world and 25% of deaths in the developing world. By the year 2020, cardiovascular disease will cause an estimated 25 million deaths worldwide, becoming the predominant cause of death in the world, surpassing infectious diseases.
Mortality and morbidity
Cardiovascular disease is the leading cause of death in the United States. Each year, approximately 500,000-700,000 deaths are attributed to coronary artery disease. About 13% of individuals with non–ST-segment elevation myocardial infarction (NSTEMI) acute coronary syndrome and 8% of those with unstable angina who reach the hospital die within 6 months, according to the Global Registry of Acute Coronary Events (GRACE). In the same period, the rate of new stroke is 1.5-3%, and the rate of rehospitalization for a further acute coronary syndrome is 17-20%.
Sex
The incidence of acute coronary syndrome demonstrates a male predominance to approximately 70 years of age, when incidences converge in both sexes.
Women are more likely than men to be older and to have more comorbid conditions at the time of first presentation. Abnormal locations of pain, nausea, vomiting, fatigue, dyspnea, and other atypical presentations are most common in women.
Young women with acute coronary syndrome should be counseled regarding the potential teratogenic effect of statins. Hormonal replacement therapy with estrogen or progesterone) should be stopped in women who present with acute coronary syndrome.
Age
The incidence of acute coronary syndrome increases with age. Older patients with acute coronary syndrome are most likely to present with atypical symptoms. Many elderly patients with acute coronary syndrome do not receive evidence-based therapies. This situation emphasizes the importance of improving quality-of-care programs to reinforce the use of therapies among elderly individuals.3
Race
No racial predilection is observed. Racial disparities in treatment and outcome have been noted.
History, Presentation, Physical Examination, and Causes
History
Factors that predispose individuals to develop acute coronary syndrome include the following:
- Age older than 70 years
- Male sex
- Diabetes mellitus
- Known history of coronary artery disease, including myocardial infarction
- Family history of premature coronary artery disease
- Hypertension
- Hyperlipidemia
- Tobacco use
Presentation
Patients with acute coronary syndrome may present with a chief symptom of pain or discomfort in the chest or left arm, particularly if it reproduced previously documented angina.
Principal presentations of unstable angina include the following findings:
- Rest angina that occurs at rest and that usually lasts >20 minutes
- New-onset angina at least as severe as Canadian Cardiovascular Society (CCS) class III (ie, marked limitation of ordinary physical activity)
- Increasing (crescendo) angina, ie, previously diagnosed angina that has become distinctly more frequent, longer in duration, or lower in threshold (ie, increased by ≥1 CCS class to at least CCS III severity)
- Shortness of breath, which might be an anginal equivalent or a symptom of heart failure.
Patients might also present with atypical symptoms, such as arm, jaw, neck, ear, or epigastric discomfort. When the symptoms are clearly related to exertion or stress or when they are promptly relieved with nitroglycerin, they could be anginal equivalents. Atypical presentations are common and frequently lead to misdiagnoses of abdominal pain, altered mental status, shock, or renal failure, for example.
Physical examination
Physical findings can vary from normal to any of the following:
- Hypotension or hypertension
- Diaphoresis
- Pulmonary edema and other signs of left heart failure
- Extracardiac vascular disease
- Fourth heart sound (S4), which may be heard in patients with ischemia or systolic murmur secondary to mitral regurgitation. (This is frequently present, especially in patients with inferior-wall ischemia.)
- Other findings (eg, cool, clammy skin and diaphoresis in patients with cardiogenic shock)
- Systolic murmur related to dynamic obstruction of the left ventricular outflow tract (This is caused by hyperdynamic motion of the basal left ventricular myocardium and may be heard in patients with an apical infarct.
Causes
The most common cause of acute coronary syndrome is coronary thrombosis on a preexisting plaque. The degree of occlusion determines the patient's subsequent presentation.
Risk factors for coronary artery disease include the following:
- Age
- Sex
- Family history of premature coronary heart disease
- Tobacco use
- Diabetes mellitus
- Hypertension
- Dyslipidemia
- Obesity, especially the male-pattern truncal form
- Peripheral vascular disease
- Previous stroke
Other causes of NSTEMI acute coronary syndrome include the following:
- Dynamic obstruction (coronary spasm or vasoconstriction)
- Cocaine or amphetamine use, which increases myocardial oxygen demand and which may cause coronary vasospasm
- Use of certain medications, such as selective serotonin reuptake inhibitors (SSRIs)
- Progressive mechanical obstruction
- Inflammation4 and/or infection
- Embolic occlusion of the coronary arteries
- Congestive heart failure
- Underlying coronary artery disease, which severe anemia or hypoxemia might precipitate
- Coronary artery dissection (spontaneous or iatrogenic)
- Coronary artery injury during blunt or penetrating chest trauma
- Coronary artery anomaly, such as a left anterior descending coronary artery originating from the pulmonary trunk or a left main coronary artery originating from the right coronary sinus of the aortic valve with a course between the great vessels
Differential Diagnoses and Other Problems to Consider
Differential diagnoses
Aortic dissection
Aortic stenosis
Esophageal spasm
Gastroesophageal reflux disease
Myocarditis
Pneumothorax
Pulmonary embolism
Other problems to consider
Acute cholecystitis
Hypertensive emergency
Panic attack
Pericarditis
Laboratory Studies
Electrocardiography
Recording an ECG during an episode of the presenting symptoms is valuable. Transient ST-segment changes (>0.05 mV) that develop during a symptomatic period and that resolve when the symptoms do is strongly predictive of underlying coronary artery disease and has prognostic value. Comparison with previous ECGs is often helpful.
Alternative causes of ST-segment and T-wave changes are left ventricular aneurysm, pericarditis, Prinzmetal angina, early repolarization, Wolff-Parkinson-White syndrome, drug therapy (eg, with tricyclic antidepressants, phenothiazines).
Measurement of cardiac enzyme levels
Measure cardiac enzyme levels at regular intervals, starting on admission and continuing until the peak is reached or until 3 sets of results are negative. Biochemical biomarkers are useful for both diagnosis and prognostication (see Media file 1).
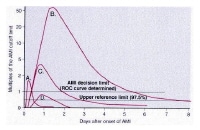
This plot shows changes in cardiac markers over time after the onset of symptoms. Peak A is the early release of myoglobin or creatine kinase isoenzyme MB (CK-MB) after acute myocardial infarction (AMI). Peak B is the cardiac troponin level after infarction. Peak C is the CK-MB level after infarction. Peak D is the cardiac troponin level after unstable angina. Data are plotted on a relative scale, where 1.0 is set at the myocardial-infarction cutoff concentration. Courtesy of Wu et al (1999). ROC = receiver operating characteristic.
Of note, cardiac-specific troponins are not detectable in the blood of healthy individuals; therefore, they provide high specificity for detecting injury to cardiac myocytes. These molecules are also more sensitive than CK-MB for myocardial necrosis and, thus, improve early detection of small myocardial infarctions. Although blood troponin levels increase simultaneously with CK-MB levels (about 6 h after the onset of infarction), they remain elevated for as long as 2 weeks. As the result, troponin values cannot be used to diagnose reinfarction. New methods of detecting troponins in the blood can measure levels as low as 0.1-0.2 ng/mL.
Minor elevations in these molecules can be detected in the blood of patients without acute coronary syndrome in the setting of myocarditis (pericarditis), sepsis, renal failure, acute congestive heart failure, acute pulmonary embolism, or prolonged tachyarrhythmias.
- Measurement of CK-MB levels
- CK-MB, the isoenzyme specific to the heart muscle, was the principal biomarker of cardiac injury until troponin supplemented it.
- In the setting of myocardial infarction, plasma CK-MB concentrations typically rise about 4-6 hours after the onset of chest pain. They peak within 12-24 hours and return to baseline levels within 24-48 hours.
- Serial measurements obtained every 6-8 hours (at least 3 times) are warranted until peak values are determined.
- Clinical settings other than acute coronary syndrome, such as trauma, heavy exertion, and skeletal muscle disease (eg, rhabdomyolysis) may elevate CK-MB values.
- The area under the concentration-time curve for CK-MB created with serial measurements of blood enzyme levels provides a reliable estimate of the size of the infarct.
- Determination of subforms of CK-MB (CK-MB2 that is more specific to heart muscle) may improve the sensitivity of this test.
- Measurement of troponin levels
- Troponin is part of the contractile apparatus of the myocyte associated with tropomyosin and actin and myosin filaments. Troponin has 3 subunits: TnT, TnI, and TnC. TnI and TnT are normally not detectable in the blood.
- Measurement of troponin level has both diagnostic and prognostic value.
- Positive troponin levels are virtually diagnostic of myocardial infarction in the most recent revisions of the ACC/AHA guidelines, as they are without equal in terms of combined specificity and sensitivity in diagnosing myocardial infarction.
- Elevated troponin levels might help in identifying patients who might greatly benefit from aggressive antiplatelet and other adjunctive therapy.5
- Troponin levels are typically measured serially along with CK values.
- Measurement of myoglobin levels
- Myoglobin is not cardiac specific, but it may be detected as early as 2 hours after myocardial necrosis starts.
- Myoglobin results should be supplemented with other more specific cardiac biomarkers, such as CK-MB or troponin.
- Myoglobin values have a high negative predictive value when blood is sampled in the first 4-8 hours after onset.
CBC determination
The CBC helps in ruling out anemia as a secondary cause of acute coronary syndrome. Leukocytosis has prognostic value in the setting of acute myocardial infarction.
Basic metabolic panel
Close monitoring of potassium and magnesium levels is important in patients with acute coronary syndrome because low levels may predispose them to ventricular arrhythmias. Routine measurement of serum potassium levels and prompt correction are recommended.
A creatinine level is also needed, particularly if cardiac catheterization is considered. Use of N -acetylcysteine and adequate hydration can help prevent contrast material–induced nephropathy.6
New biomarkers
Levels of brain natriuretic peptide (BNP) and N-terminal pro-BNP (NT-pro-BNP) are elevated in acute MI and provide predictive information for risk stratification across the spectrum of acute coronary syndrome.7,8
In the future, a combination of levels of troponin (a biomarker of myocardial necrosis), NT-pro-BNP (an indicator of elevated left ventricular end-diastolic pressure and wall stress), and C-reactive protein (CRP, an estimate of extent of systemic inflammation) may prove useful for predicting the outcome of patients with acute coronary syndrome.
Routine measurement of BNP and CRP levels in patients with acute coronary syndrome is not warranted at this time.
Imaging Studies
Chest radiography
Chest radiography helps in assessing cardiomegaly and pulmonary edema. A chest radiograph may also assist in diagnosing concomitant disease (eg, pneumonia in an elderly patient) as a precipitating cause of acute coronary syndrome.
Echocardiography
An echocardiogram may play an important role in the setting of acute coronary syndrome. Regional wall-motion abnormalities can be identified. Echocardiograms are especially helpful if the diagnosis is questionable.
An echocardiogram can also help in defining the extent of the infarction and assess overall function of the left and right ventricles. In addition, an echocardiogram can help identify complications such as acute mitral regurgitation, left ventricular rupture, and pericardial effusion.
Absence of segmental wall-motion abnormality on echocardiography during active chest discomfort is a highly reliable indicator of a nonischemic origin of symptoms.
Myocardial perfusion imaging
Myocardial perfusion is a valuable method for triaging patients with chest pain in the emergency department. Myocardial perfusion imaging at rest is highly sensitive for detecting acute myocardial infarction, and it can be supplemented with provocative testing after infarction is excluded.
Results of clinical trials can be applied only in centers with proven reliability and experience.
The sensitivity of single photon emission computed tomography (SPECT) is sufficient to detect infarcts of at least 10 g, but MRI with gadolinium enhancement may depict infarcts as small as 1–5 g.
Cardiac angiography
Cardiac catheterization helps in defining the patient's coronary anatomy and the extent of the disease.
Patients with cardiogenic shock, intractable angina despite medication, severe pulmonary congestion, or right ventricular infarction should immediately undergo cardiac catheterization.
For high-risk patients with acute coronary syndrome without persistent ST elevation, angiography with glycoprotein IIb/IIIa inhibition has been recommended.
Most patients benefit from angiography when they have a TIMI risk score of less than 3 points (see Table).
Table
Characteristic
| Risk Score
|
History
|
Age ≥65 y
| 1
|
At least 3 risk factors for coronary heart disease
| 1
|
Previous coronary stenosis ≥50%
| 1
|
Use of aspirin in previous 7 d
| 1
|
Presentation
|
At least 2 anginal episodes in the previous 24 h
| 1
|
ST-segment elevation on admission ECG
| 1
|
Elevated levels of serum biomarkers
| 1
|
Total score
| 0-7
|
Characteristic
| Risk Score
|
History
|
Age ≥65 y
| 1
|
At least 3 risk factors for coronary heart disease
| 1
|
Previous coronary stenosis ≥50%
| 1
|
Use of aspirin in previous 7 d
| 1
|
Presentation
|
At least 2 anginal episodes in the previous 24 h
| 1
|
ST-segment elevation on admission ECG
| 1
|
Elevated levels of serum biomarkers
| 1
|
Total score
| 0-7
|
Note—Event rates significantly increased as the TIMI risk score increased in the test cohort in the TIMI IIB study. Rates were 4.7% for a score of 0/1, 8.3% for 2, 13.2% for 3, 19.9% for 4, 26.2% for 5, and 40.9% for 6/7 (
P < .001, χ
2 test for the trend). The pattern of increasing event rates with increasing TIMI risk score was confirmed in all 3 validation groups (
P < .001).
After the diagnosis of acute coronary syndrome is established, risk stratification based on TIMI risk scores and the GRACE risk of death can be useful in making clinical decisions regarding the need for an invasive approach. Patients are at higher risk if the following findings are present:
- Clinical instability
- Accelerating chest pain in the 48 hours before presentation
- Prolonged ischemic chest pain
- Clinical evidence of heart failure
- Hypotension
- Ventricular tachycardia
- ECG changes of ischemia
- Positive cardiac biomarkers
- TIMI risk score of more than 3 points (see the Table above) or a GRACE risk of death more than 4%.
Medical Care and Coronary Interventions
Medical Care
- Initial therapy for acute coronary syndrome should focus on stabilizing the patient's condition, relieving ischemic pain, and providing antithrombotic therapy to reduce myocardial damage and prevent further ischemia.
- Morphine (or fentanyl) for pain control, oxygen, sublingual and/or intravenous nitroglycerin, soluble aspirin 162-325 mg, and clopidogrel with a 300- to 600-mg loading dose are given as initial treatment.
- Humidified oxygen may reduce the risk of nosebleeds in patients with acute coronary syndrome who are receiving antiplatelet and antithrombin therapy.
- Do not administer nitrates if the patient is hypotensive (systolic BP <90>
- Patients with known hypersensitivity to antiplatelet agents, active internal bleeding, and bleeding disorders should not receive antiplatelet or antithrombotic therapy.
- High-risk patients with non–ST-segment elevation myocardial infarction (NSTEMI) acute coronary syndrome should receive aggressive care, including aspirin, clopidogrel, unfractionated or low molecular weight heparin (LMWH), intravenous platelet glycoprotein IIb/IIIa complex blockers (eg, tirofiban, eptifibatide), and a beta-blocker. The goal is early revascularization.
- Intermediate–risk patients with NSTEMI acute coronary syndrome should rapidly undergo diagnostic evaluation and further assessment to determine their appropriate risk category.
- Low-risk patients with NSTEMI acute coronary syndrome should undergo further follow-up with biomarkers and clinical assessment. Optimal medical therapies include use of standard medical therapies, including beta-blockers, aspirin, and unfractionated heparin or LMWH. The CURE study has shown that clopidogrel would be beneficial even in low-risk patients.10 If no further pain occurs, and follow-up studies are negative, a stress study should drive further management.
- First-line therapy in patients with chest pain regardless of their risk strategy includes a combination of oxygen, aspirin, nitroglycerin, and morphine.
- Mehta et al studied 3031 patients with acute coronary syndromes. Early intervention (coronary angiography £ 24 h after randomization; median time 14 h) in acute coronary syndromes did not differ greatly from delayed intervention (coronary angiography >24 h randomization; median time 50 h) in preventing the primary outcome (ie, composite of death, myocardial infarction, or stroke at 6 mo). Early intervention did reduce the rate of the secondary outcome (ie, death, myocardial infarction, or refractory ischemia at 6 mo) and improved the primary outcome in patients who were at highest risk (ie, Global Registry of Acute Coronary Events [GRACE] risk score >140).11
Anti-ischemic therapy
Nitrates12 do not improve mortality. However, they provide symptomatic relief by means of several mechanisms, including coronary vasodilation, improved collateral blood flow, decrease in preload (venodilation and reduced venous return), and decrease in afterload (arterial vasodilation). Care should be taken to avoid hypotension because this can potentially reduce coronary perfusion pressure (diastolic BP - left ventricular diastolic pressure).
Beta-blockers are indicated in all patients unless they have the following contraindications:
- Hypotension
- Shock
- Severe bradycardia
- High-grade atrioventricular block
- Severe obstructive pulmonary disease
Beta-blockers reduce oxygen demand and ventricular wall tension. They also decrease mortality and adverse cardiovascular events. These drugs may prevent mechanical complications of myocardial infarction, including rupture of the papillary muscle, left ventricular free wall, and ventricular septum. Beta-blockers meliorate dynamic obstruction of the left ventricular outflow tract in patients with apical infarct and hyperdynamic basal segments.
The most frequently used regimen is intravenous metoprolol 2-5 mg given every 5 minutes (up to 15 mg total) followed by 25-100 mg given orally twice a day.
Beta-blockers should not be used acutely in patients with cardiogenic shock or signs of heart failure on presentation.
Antithrombotic therapy
Aspirin permanently impairs the cyclooxygenase pathway of thromboxane A2 production in platelets and, thus, inhibits platelet function. Aspirin reduces morbidity and mortality and is continued indefinitely.13
Clopidogrel (thienopyridine) inhibits adenosine 5'-diphosphate (ADP)–dependent activation of the glycoprotein IIb/IIIa complex, a necessary step for platelet aggregation. This process results in intense inhibition of platelet function, particularly in combination with aspirin. In the Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) trial, thienopyridine reduced the rate of myocardial infarction by 20%.
Clopidogrel is a class I recommendation for patients when early noninterventional approach is planned in therapy for at least 1 month to as long as 9 months.14 When percutaneous coronary intervention (PCI) is planned, clopidogrel is started and continued for at least 1 month and up to 9 months, if the patient is not at high risk for bleeding.
The optimal dosage for clopidogrel is still being evaluated. Reports show that a loading dose of 600 mg might be more beneficial than 300 mg. Withhold clopidogrel for at least 5 days before elective coronary artery bypass grafting (CABG). Since 12% of patients with non-ST elevation acute coronary syndrome have coronary anatomy that favors CABG, use of clopidogrel is withheld until coronary angiography at some institutions.
The TRITON TIMI 38 trial studied patients with acute coronary syndromes with scheduled percutaneous coronary intervention. Prasugrel therapy was associated with significantly reduced rates of ischemic events, including stent thrombosis, but with an increased risk of major bleeding, including fatal bleeding. Overall mortality did not differ significantly between treatment groups.15
Ticagrelor is the first reversible oral P2Y receptor antagonist. It provides faster, greater, and more consistent adenosine diphosphate–receptor inhibition than clopidogrel, and is being studied in the PLATO trial.16
Glycoprotein IIb/IIIa receptor antagonists include abciximab17,18 , eptifibatide19 , and tirofiban20 . These drugs inhibit the glycoprotein IIb/IIIa receptor, which is involved in the final common pathway for platelet adhesion and aggregation.
Two trials with tirofiban and 1 trial with eptifibatide have also documented their efficacy in unstable angina/NSTEMI patients, only some of whom underwent interventions. These antagonists are a class I recommendation in patients where catheterization and PCI are planned. Intermediate- and high-risk patients appear to respond favorably to glycoprotein IIb/IIIa inhibitors.21 They include patients with ST-segment depression, elevated risk scores, elevated serum troponin levels22 , and/or diabetes mellitus.
Use eptifibatide or tirofiban in patients with high-risk features in whom invasive treatment is not planned.
The EARLY ACS trial compared a strategy of early, routine administration of eptifibatide with delayed, provisional administration in patients who had acute coronary syndromes without ST-segment elevation and who were assigned to an invasive strategy. The use of eptifibatide 12 hours or more before angiography was not superior to the provisional use of eptifibatide after angiography, and early use of eptifibatide was associated with an increased risk of non–life-threatening bleeding and need for transfusion.23
Anticoagulation
Unfractionated heparin was associated with a 33% reduction in the risk of myocardial infarction or death in patients with unstable angina who were treated with aspirin plus heparin compared with aspirin alone.24
LMWHs might be superior to heparin in reducing cardiovascular outcomes with a safety profile similar to that of heparin in patients receiving medical care.
Nine randomized trials have directly compared LMWH with unfractionated heparin. Two trials evaluated dalteparin, another evaluated nadroparin, and 6 evaluated enoxaparin.25,26 Heterogeneity of trial results has been observed. Trials with dalteparin and nadroparin reported similar rates of death or nonfatal myocardial infarction compared with heparin, whereas 5 of 6 trials of enoxaparin found point estimates for death or nonfatal myocardial infarction that favored enoxaparin over heparin. The benefit of enoxaparin appeared to be driven largely by a reduction in nonfatal myocardial infarction, especially in the cohort of patients who had not received any open-label anticoagulant therapy before randomization.
The role of LMWHs in patients for whom PCI is scheduled is relatively ill defined. However, it is likely to be at least equivalent to that of heparin. It appears reasonable to minimize the risk of excessive anticoagulation during PCI by avoiding crossover of anticoagulants (ie, maintain consistent anticoagulant therapy from the pre-PCI phase throughout the procedure itself). Additional experience with regard to the safety and efficacy of the concomitant administration of LMWHs with GP IIb/IIIa antagonists and fibrinolytic agents is currently being acquired.
Current guidelines for patients with moderate- or high-risk acute coronary syndromes recommend an early invasive approach with concomitant antithrombotic therapy, including aspirin, clopidogrel, and unfractionated or low-molecular-weight heparin. The ACUITY trial evaluated the role of thrombin-specific anticoagulation with bivalirudin in this patient population. In patients with moderate- or high-risk acute coronary syndromes who were undergoing invasive treatment with glycoprotein IIb/IIIa inhibitors, bivalirudin was associated with rates of ischemia and bleeding that were similar to those with heparin. Bivalirudin alone was associated with similar rates of ischemia and significantly lower rates of bleeding.27 Further, glycoprotein IIb/IIIa inhibitors can be initiated at the time of angiography; routine administration 12-24 hours before the procedure carries an increased risk of bleeding and no improvement in outcome.
In summary, for patients in whom an invasive strategy is selected, regimens with established efficacy include enoxaparin and unfractionated heparin (Class I, Level of Evidence: A) and bivalirudin and fondaparinux (Level of Evidence: B). For patients in whom a conservative strategy is selected, regimens using either enoxaparin or UFH (Class I, Level of Evidence: A) or fondaparinux (Level of Evidence: B) have established efficacy. In patients in whom a conservative strategy is selected and who have an increased risk of bleeding, fondaparinux is preferable (Level of Evidence: B).
For unstable angina/NSTEMI patients in whom an initial conservative strategy is selected, fondaparinux is preferable to UFH as anticoagulant therapy unless CABG is planned within 24 hours (Class IIa, Level of Evidence: B).
Thrombolysis
Thrombolysis has no role in NSTEMI acute coronary syndrome.
Coronary Interventions
An early invasive strategy is indicated in unstable angina/NSTEMI patients who have refractory angina or hemodynamic or electrical instability without serious comorbidities or contraindications to such procedures (Class I). An early invasive strategy is also indicated in initially stabilized unstable angina/NSTEMI patients without serious comorbidities or contraindications to such procedures who have an elevated risk for clinical events (Class I). In NSTEMI acute coronary syndrome , early revascularization reduces myocardial infarction and death rates compared with a more selective strategy, particularly in high-risk patients. Use of glycoprotein IIb/IIIa blockers followed by early invasive catheterization is the most logical approach. An early invasive strategy should be considered in patients with large myocardial infarction, hypotension, shock, right ventricular infarction, and refractory chest pain.
Further Patient Care
Consultations
- Emergency department personnel should be well aware of the initial evaluation, triaging, and treatment of patients with chest pain (see Media file 2).

Suggested algorithm for triaging patients with chest pain. ACS = acute coronary syndrome; ASA = aspirin; EKG = ECG; MI = myocardial infarction; Rx = treat; STEMI = ST-elevation myocardial infarction. Courtesy of Wu et al (1999).
- Internists manage many cases of acute coronary syndrome.
- Have a low threshold for consulting cardiologists, particularly if the patient has high-risk acute coronary syndrome and if cardiac catheterization is being considered.
Diet
- Patients should receive nothing by mouth (NPO) until their condition is stabilized and treated.
- Maintain the patient's NPO status from midnight before cardiac catheterization if it is being considered.
- After initial therapy and admission, a dietitian should instruct the patient regarding an appropriate diet, as recommended by the AHA. A low-salt, low-fat, and low-cholesterol diet is generally recommended.
Activity
- Limit patients to bed rest to minimize their oxygen consumption until reperfusion and initial therapy are complete. After that, the patient's activity may slowly be increased as tolerated and as the clinical situation allows.
- Start cardiac rehabilitation before the patient is discharged.
Further inpatient care
Patients may receive additional care in a telemetry-monitored unit if their condition is stable. Carefully monitor patients for arrhythmia, recurrent ischemia, and other possible complications. If patients have not undergone cardiac catheterization and if they have no complications, an ischemia-driven approach to PCI can be taken.
Further outpatient care
Arrange for follow-up within 2 weeks of the patient's discharge.
Inpatient and outpatient medications
- Long-term use of aspirin in patients who have had a myocardial infarction significantly reduces the subsequent risk of death.
- Clopidogrel, along with aspirin, should be prescribed for at least 9 months after discharge if the patient has no contraindications. To reduce the risk of bleeding, the dose of aspirin can be reduced to 81 mg.
- In 2009, Ho et al reported on clopidogrel use after hospital discharge in a retrospective cohort study of more than 8000 patients with acute coronary syndrome. The authors determined that the use of clopidogrel concomitantly with proton pump inhibitors is associated with an increased risk of adverse outcomes, including death, compared with the use of clopidogrel alone. These results indicate that proton pump inhibitors may reduce the benefits of clopidogrel after acute coronary syndrome.28
- If aspirin cannot be tolerated, clopidogrel is the antiplatelet drug of choice.
- Beta-blocker therapy has confirmed therapeutic benefits in survivors of acute myocardial infarction. This therapy is most beneficial in patients with the highest risk.
- Many trials have shown a clear benefit of lipid-lowering therapy in the primary and secondary prevention of coronary artery disease.29
- The National Cholesterol Education Panel has set guidelines for target cholesterol levels. In general, patients who have had a myocardial infarction should achieve a low-density lipoprotein cholesterol (LDL) level less than 100 mg/dL, a high-density lipoprotein cholesterol (HDL) level greater than 40 mg/dL, and a triglyceride level less than 200 mg/dL. High-risk patients should be treated to a target LDL level of less than 70 mg/dL.
- In the Myocardial Ischemia Reduction with Aggressive Cholesterol Lowering (MIRACL) trial, Schwartz et al showed that starting atorvastatin during hospitalization for an acute coronary syndrome, irrespective of lipid levels, reduces the frequency of recurrent ischemic events.30 This treatment significantly reduced the frequency of the combined end point of death, recurrent death, myocardial infarction, or worsening unstable angina requiring hospitalization.
- The Pravastatin or Atorvastatin Evaluation and Infection Therapy (PROVE-IT)–Thrombolysis in Myocardial Infarction (TIMI) 22 trial showed that the use of intensive statin therapy versus standard therapy improved clinical outcomes over 2 years in patients with acute coronary syndrome.
Transfer
Patients with acute coronary syndrome with high-risk features should be transferred to a facility where catheterization is available. Start eptifibatide or tirofiban with other medical therapy, and transfer the patient to a facility where PCI can be performed.
Complications and Prognosis
Complications
Monitor and immediately treat arrhythmias in the first 48 hours. Pay attention to exacerbating factors, such as disturbances in electrolytes (especially potassium and magnesium), hypoxemia, drugs, or acidosis. Correct these factors accordingly.
Recurrent ischemia may be due to incomplete reperfusion. In the setting of PCI, consider stent thrombosis as a possible cause. Whether drug-eluting stents have an increased rate of thrombosis compared with bare metal stents is unclear.
CHF can be due to systolic dysfunction or diastolic dysfunction in the setting of myocardial infarction. Aggressive treatment is indicated to prevent worsening of the situation.
Cardiogenic shock is defined as a systolic BP less than 90 mm Hg in the presence of organ hypoperfusion. This finding is associated with a high mortality rate. Pressor agents, such as dopamine, and inotropic agents, such as dobutamine, may be needed.
Some patients with intractable chest pain or severe hypotension may require the insertion of an intra-aortic balloon pump. The EuroHeart survey showed a nearly 40% reduction in the risk for death in patients with acute coronary syndrome who received support with an intra-aortic balloon pump. This benefit was independent of the status of the ST segment.
Patients presenting with cardiogenic shock should undergo PCI as soon as possible.
Prognosis
Six-month mortality rates in the GRACE registry were 13% for patients with NSTEMI acute coronary syndrome and 8% for those with unstable angina.
Patient Education
The mnemonic ABCDE might be helpful.
- A = Aspirin and antianginals
- B = Beta-blockers and BP
- C = Cholesterol and cigarettes
- Educate all patients who have had a myocardial infarction about the critical role of smoking in the development of coronary artery disease.
- Smoking-cessation classes should be offered to help patients avoid smoking after a myocardial infarction.
- Cigarette smoking is a major risk factor for coronary artery disease. The risk of recurrent coronary events decreases 50% at 1 year after smoking cessation.
- Provide all patients who smoke with guidance, education, and support to avoid smoking.
- Bupropion increases the likelihood of successful smoking cessation.
- D = Diet and diabetes
- Diet plays an important role in the development of coronary artery disease.
- Educate patients who have had a myocardial infarction about the role of a low-cholesterol and low-salt diet.
- Educate patients about AHA dietary guidelines regarding a low-fat, low-cholesterol diet.
- A dietitian should see and evaluate all patients who have had a myocardial infarction before they are discharged.
- E = Exercise and education
- A cardiac rehabilitation program after discharge might reinforce education and enhance compliance.
- Failure to diagnose a myocardial infarction is the leading cause of litigation against emergency physicians and cardiologists.
- Consider the possibility of atypical presentations in women, elderly patients, and patients with diabetes.
- ECGs should be reviewed promptly.
- Early imaging is useful to assess wall-motion abnormalities in difficult cases with nondiagnostic ECGs, such as those involving a left bundle-branch block.
- Involve a cardiologist when in doubt.
Special Concerns
- Elderly patients
- Elderly patients are at increased risk for adverse outcomes.
- Decisions about their care should reflect considerations of their general health, cognitive status, and life expectancy.
- Altered pharmacokinetics and sensitivity to drugs are other issues to be considered.
- Women
- Women with acute coronary syndrome should be cared for as men are.
- Like their male counterparts, women with unstable angina and/or NSTEMI should receive aspirin and clopidogrel.
- Indications for testing are similar in men and women.
- Patients with diabetes mellitus
- Outcomes are worse in patients with diabetes than in those without diabetes.
- Tight glycemic control should be maintained.
- Patients who have undergone CABG
- Medical treatment should follow the same guidelines as those established for patients who have not undergone CABG.
- Have a low threshold for catheterization in patients with acute coronary syndrome who underwent CABG.
- Patients with cocaine use
- Give nitroglycerin and oral calcium antagonists for patients with STEMI or depression that accompanies chest discomfort.
- Immediately perform catheterization if ST elevation persists after the administration of nitroglycerin and calcium channel blockers.
- Patients with Prinzmetal angina
- Perform angiography in patients with episodic chest pain and ST-segment elevation that resolves with nitroglycerin and/or calcium channel blockers.
- Administer nitrates and calcium channel blockers in patients whose catheterization does not show obstructive coronary artery disease.
- Patients with syndrome X
- Offer reassurance, and provide medical therapy with nitrates, beta-blockers, and calcium channel blockers alone or in combination.
- Reduce risk factors.
Multimedia
| Media file 1: This plot shows changes in cardiac markers over time after the onset of symptoms. Peak A is the early release of myoglobin or creatine kinase isoenzyme MB (CK-MB) after acute myocardial infarction (AMI). Peak B is the cardiac troponin level after infarction. Peak C is the CK-MB level after infarction. Peak D is the cardiac troponin level after unstable angina. Data are plotted on a relative scale, where 1.0 is set at the myocardial-infarction cutoff concentration. Courtesy of Wu et al (1999). ROC = receiver operating characteristic. |
| Media file 2: Suggested algorithm for triaging patients with chest pain. ACS = acute coronary syndrome; ASA = aspirin; EKG = ECG; MI = myocardial infarction; Rx = treat; STEMI = ST-elevation myocardial infarction. Courtesy of Wu et al (1999). |
Keywords
acute coronary syndrome, ACS, myocardial infarction, MI, ST-segment elevation myocardial infarction, STEMI, non–ST-segment elevation myocardial infarction, NSTEMI, coronary artery disease, CAD, unstable angina, UA, transmural MI, nontransmural MI, subendocardial MI, cardiovascular disease, CVD, chronic heart failure, congestive heart failure, CHF, coronary heart disease, CHD.
Source : http://emedicine.medscape.com/article/164525-overview?src=emed_whatnew_nl_0#EarlyIntervention






